I - PK (Pharmaco-Kinetics):1. ADME:
Absorption,
Distribution,
Metabolism,
Excretion
2. Absorption mechanism: pinocytosis, passive diffusion, active transport, facilitated diffusion
3. Terms:
Bioavailability = %[drug]systemic circulation
Bioequivalence = same AUC (Cmax, Tmax)
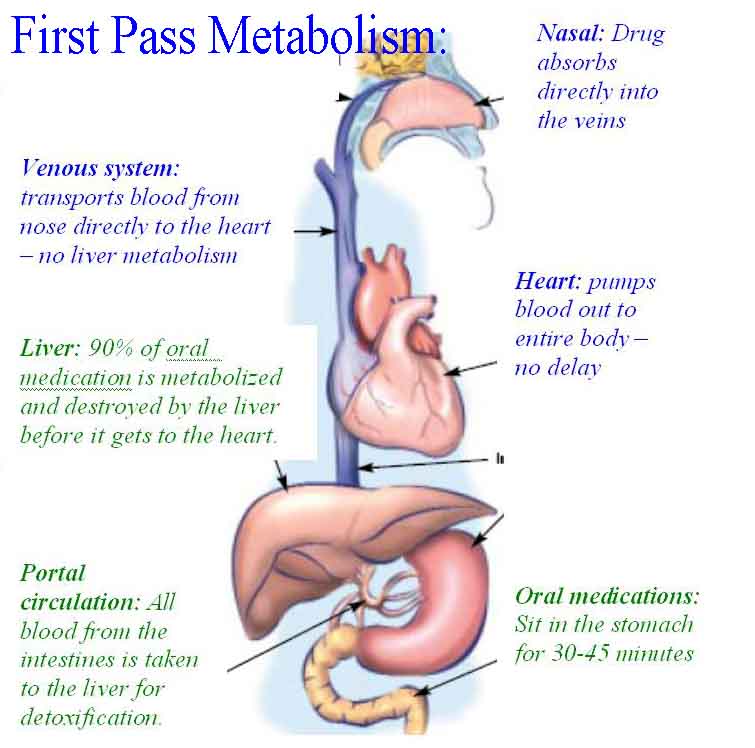
First-pass effect = oral then after liver
Volume of distribution = dose/[plasma concentration]
Clearance = t(totally eliminated)
Area under the Curve (AUC) = Cmax, total T(drug exposure)
Cmax = max [drug]blood (i.e., max drug conc. in blood)
Tmax = time 'til Cmax (i.e. time it takes for Cmax to occur)
Half-life (t1/2) = time until 50% of drug is eliminated from body
Steady state: 3-5 half-lives
Elimination time: 4-5 half-lives
II - PD (Pharmaco-Dynamics):1. Receptor types:
a.
Gated-ion channels: agonist => opens channels. Ex: ACh (Nicotinic), GABA (anti-stress, anti-anxiety), 5-HT (serotonin - antidepressant)
b.
G-protein coupled: α,
β adrenergic
c.
Transmembraneous: insulin, peptide
d.
Intracellular: sex hormones, glucocorticoids
2.
Drug - receptor interactions: a.
affinity: strength of binding to receptors
b.
potency: high potency = lower dose for effects
c.
efficacy: high efficacy =
3. Drug dose:
a.
ED50: effective dose in 1/2 of pts
b.
TD50: toxic dose in 1/2 pts
c.
LD50: lethal dose in 1/2 pts
d.
TI = TD50/ED50: therapeutic index
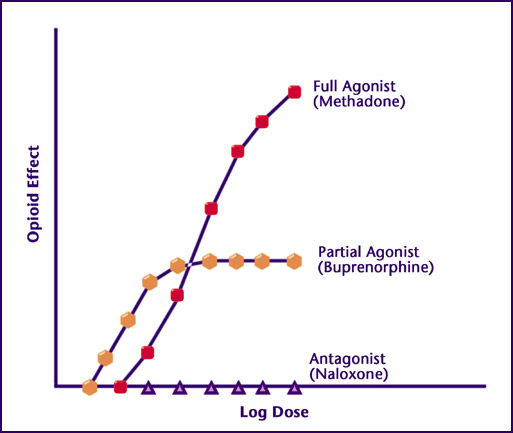
4.
Agonist: a.
Full: full effects
b.
Partial: less than full effects
c.
Full agonist + partial agonist = partial acts as INHIBITOR
5.
Antagonist: a.
Pharmacologic: binds to block receptors. Ex: propanolol as beta-blockers
b.
Competitive: replace-able if higher conc. of agonist. Ex: naloxone for opioid receptors
c.
Irreversible: non-replace-able even if higher conc. of agonist. Ex: Phenoxybenzamine as adreno-receptors antagonists.
d.
Physiologic: binds to opposite receptors to produce opposite effects. Ex: epinephrine for antihistamines effects
III - Adverse Drug Reactions: 1. Drug-drug
2. Dose-related
3. Disease-related
4. Side effect
5. Intolerance (sensitivity)
6. Toxicity
7. Drug allergies
IV - Scheduled drugs:1.
Schedule I: nobody can prescribe, highest abuse Ex: heroin, Marijuana, LSD, Peyote, Ecstasy, Quaalude
2.
Schedule II: hand-delivered paper signature prescriptions Ex: Vicodin, cocaine
3.
Schedule III: fax prescription Ex: codeine/acetaminophen, anabolic steroids (oxa-drolone), didrex (benzphatamine), oral marinol.
4.
Schedule IV: fax prescription Ex: tramadol, sleeping pills (bensolam, ambien), BZD (valium), soma, etc.
5.
Schedule V: fax prescription Ex: Lomotil, Phenergan with Codeine, Robitussin with codeine, AED (vimpat, Lyrica, ezogabine)
6.
CURES: II, III, IV drug registry in California
V - Prescription Writing:1. sig., #refills, DAW?
2. Do NOT use list
VI - FDA Drug approval process: 1. Discovery
2. Animal-testing
3. Clinical trials:
a. Phase 1: 20-100 healthy persons (PK)
b. Phase 2: 100-200 target disease pts (efficacy, not by chance)
c. Phase 3: 1000's target disease pts (safety for lots, not just efficacy)
d. Phase 4 (optional): 100,000 target disease pts (maybe some bad side effects in phase 3, not known long enuf in phase 3, most likely the public will be unlikely to use it ...)
4. Post-marketing surveillance:
a.
REMS: FDA programs to ensure drug use is approrpiate (Mifeprex, Acne drug)
b. MedWatch, 'Dear Heath Care Professionals' letters: Auvi-Q, certain albuterol inhalers
VII - Drug names:1. Chemical: IUPAC
2. Generic: 1 for all various brand-name
3. Trade: brand names
VIII - Drug development history:1.
Pure food & drug act: bans adulteration/mislabeling
2. Food, Drug, Cosmetic act: requires tests safety & purity
3. Kefauver-Harris: requires efficacy
4. Abuse prevention: requires scheduled
5. Poison prevention: requires child-resistant
6. Orphan: incentives for rare-disease drugs
7. Prescription marketing: bans drug samples sales
8. Dietary supplement: non-FDA regulated supplements
9. FDA ammendments: FDA regulates drug commercials
10. FDA innovation: FDA accelerates break-thru & fast-track drugs
Resources:
MCQ:http://accesspharmacy.mhmedical.com/book.aspx?bookid=1576 http://global.oup.com/uk/orc/pharmacy/ifp_therapeutics/student/mcqs/ch01/http://media.pharmacologycorner.com/wp-content/uploads/2009/01/usmle-pharmacology-quiz-multiple-choice.pdfhttps://archive.org/stream/1GeneralPharmacologyMCQS/1%20General%20Pharmacology%20MCQS_djvu.txthttps://books.google.com/books?id=QlTUZH39lTYC&pg=PA13&lpg=PA13&dq=bioavailability+mcq&source=bl&ots=d9ocUgGr7A&sig=V5RMoGouHB0Yevpv2ztcsUkOC0s&hl=en&sa=X&ved=0ahUKEwi41O7MxvHLAhWru4MKHRHAATQQ6AEIMjAD#v=onepage&q=bioavailability%20mcq&f=false https://books.google.com/books?id=7PXn6BVhtT0C&pg=PA9&dq=%22competitive+antagonist%22+naloxone&hl=en&sa=X&ved=0ahUKEwjJqOTP2_HLAhUKlYMKHTFACO0Q6AEIJTAA#v=onepage&q=%22competitive%20antagonist%22%20naloxone&f=falsehttp://glutxi.umassmed.edu/documents/PharmacoDynamics.pdf ~Wonder Me